‘I have a passion for palliative care’
Doctors’ focus on curing people and prolonging their lives is stopping us from dying good deaths, says Eric Geijteman, who conducted a study on the use of medicines and other interventional medical procedures during the final stages of patients’ lives. Last week he was awarded a PhD for a thesis entitled Decisions About Medical Treatment in the Last Phase of Life.
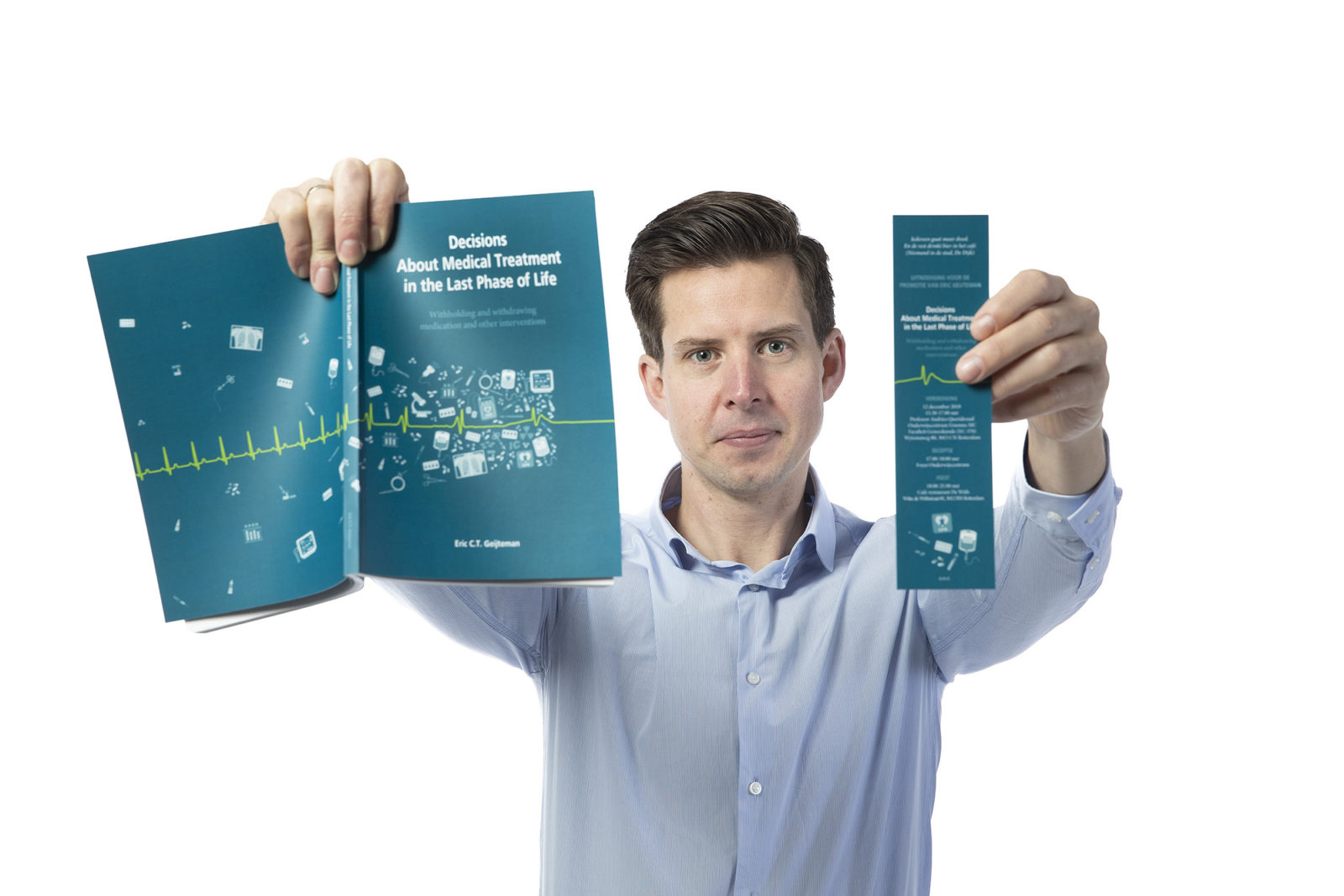
Image by: Levien Willemse
What did your study entail?
“We conducted research on interventional medical procedures performed in the last few days or weeks of a person’s life. We mainly focused on the use of medications. It’s understandable that patients take a tremendous number of medicines during their final week, since they tend to have a lot of symptoms. On the other hand, they are also administered a lot of medications during that week whose added value is either insignificant or nil. For that reason, we also conducted research on how health care providers, patients and their relatives feel about taking those medications – on their thoughts and opinions. How do they feel about some medicines being administered right until the moment of death?”
What was the main conclusion of your study?
“The focus on curing people and prolonging their lives is stopping us from dying good deaths. Professional literature shows that health care providers are completely focused on treatment and find it hard to come to terms with the idea that their patients will be dying soon. On the other hand, some patients may feel like they are being abandoned when a doctor decides not to prescribe medications any longer, as if the doctors are throwing in the towel. It’s important to consider how to have that conversation with them.
“You can explain that stopping the meds may result in the patient’s having less difficulty taking all the meds and that the risk of side-effects will be reduced. The same is true for other interventional procedures, such as ultrasound tests, imaging tests, blood tests and examinations. You can actually do a lot for patients by deciding not to do certain things. You can give them a different type of hope. Not the hope of being cured, but of, say, dying a good death.”
‘I’m not a spiritual person […] but during the evenings I worked on that particular chapter, I always had a candle burning.’
You wrote in your dissertation that you have a passion for palliative care. How did you come by this passion?
“After being unlucky in the medical school’s admissions lottery, I studied nursing for two years. During a five-month work placement at a hospital, I nursed many patients with limited life expectancy. I was attracted to that, and I’ve been mentally preoccupied with it ever since. Even then I sometimes found myself wondering: why are we doing this? As a nurse, you’re in a good position to see when a person is deteriorating. Sometimes you’ll notice it before a doctor does. That’s why it’s so important that doctors and nurses collaborate. During my medical degree, I volunteered as a carer in hospice care. After my graduation I looked for a place where I’d be able to conduct research on palliative care. After working on a report on euthanasia at Erasmus MC for a year and a half, some funds were allocated to a study on the use of medicines during the dying stages of patients’ lives. Some people think I’m crazy for being so interested in palliative care, but in the end we all die. I’ll never succeed, but what I’d like to do is try and ensure that everyone dies a good death.”
One of the chapters in your dissertation is about your father’s death. Do you wish to say anything about that?
“I was halfway through this dissertation when he passed away. The cardiologist, with whom we spoke five days before his passing, said later that he suspected straight away that [my father] would not last much longer. Even so, he tried everything he could do to save him in those final days. [My father] underwent abdominal ultrasonography twelve hours before his death. He had to hold his breath to get it done, even though he wasn’t actually capable of doing that anymore. I was in the room with him, and it was terribly undignified. Such interventional procedures not only have physical effects, but emotional and existential ones, as well, because, among other things, you are giving people hope, while at the same time robbing them of a good death. Writing about it helped me deal with my emotions. I’m not a spiritual person, and I’ve never told this to anyone, but during the evenings I worked on that particular chapter, I always had a candle burning. I shed a lot of tears while writing it. His death was an even stronger incentive to work towards giving the greatest possible number of people the best possible end of life over the next few decades. It’s incredibly rough, but at the same time I’m proud of writing such a wide-ranging dissertation.”
What’s on the cover?
“The illustrator tried to express the fact that the closer a patient is to death, and the weaker his pulse, the more interventional procedures will be performed.”
De redactie
-
 Tara Lewis
Tara LewisAuteur
Latest news
-

Agreements on international students now officially formalised
Gepubliceerd op:-
Education
-
Internationalisation
-
-

Looking for Woudestein’s wildlife with nature expert Jacob Molenaar
Gepubliceerd op:Article type: Video-
EM TV
-
-

Student union starts petition against increase in tuition fees for international students
Gepubliceerd op:-
Money
-


Comments
Comments are closed.
Read more in The PhD Defence
-

How investment treaties undermine the voices of local communities
Gepubliceerd op:-
The PhD Defence
-
-
Why it is hard to find a connection between the psychiatric illness and the brain
Gepubliceerd op:-
The PhD Defence
-
-

Dogs bring people with epilepsy their medicine when they can’t do it themselves
Gepubliceerd op:-
The PhD Defence
-